Homeless: Pipeline Problems

Why help exists on paper but breaks on the street
Voice & Vision | Homelessness and the Public Commons, Part 6 | Service delivery and bottlenecks
Part 5, The Governance Trap
Most people assume homelessness is mainly a question of will. If you cared enough, you’d fix it. If government funded it enough, it would go away. If people wanted help, they’d take it.
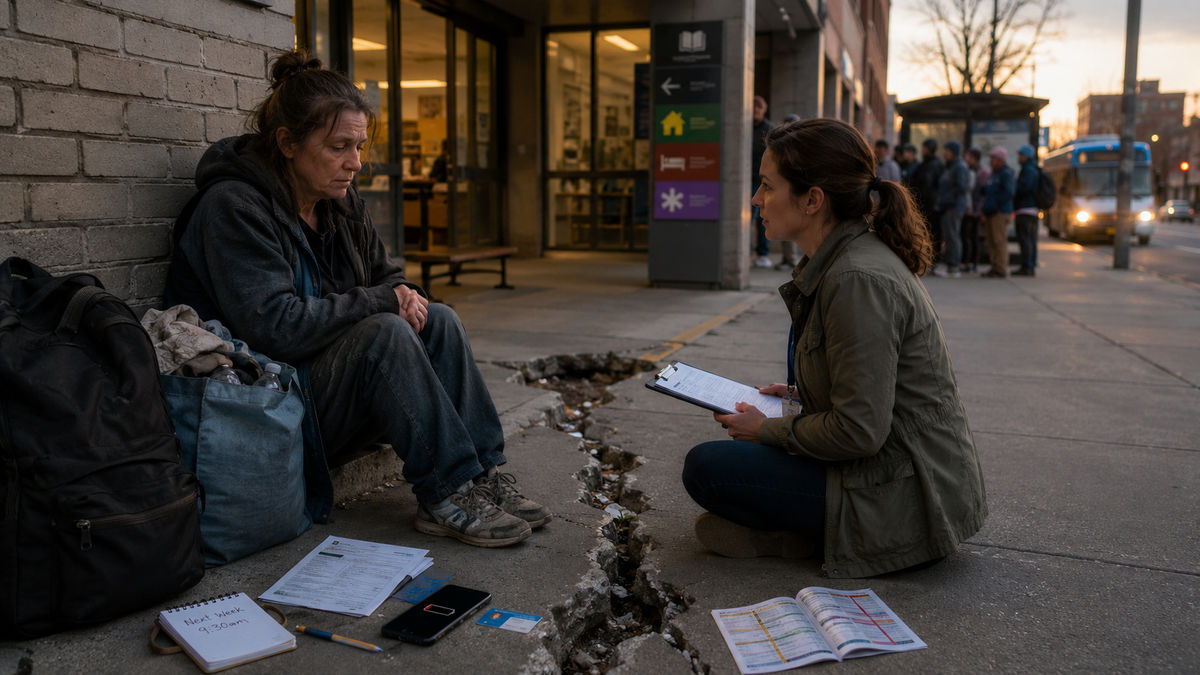
That assumption sounds reasonable until you watch how the system actually functions on the ground. Here’s a scene I keep coming back to. A woman sits outside a library with all her belongings in two bags. She looks tired, not wild. She isn’t shouting. She isn’t performing crisis. She’s just worn down. An outreach worker sits a few feet away, respectful and careful. They talk like two people trying to solve a problem that keeps changing shape.
The outreach worker offers a shelter option, but it’s across town. The woman says she tried that shelter before and got her bag stolen. The outreach worker offers another shelter, but it separates couples and she won’t leave her partner. The outreach worker offers a program intake appointment, but it’s next week, and she has no phone to confirm it and no place to keep paperwork safe. The outreach worker says there’s a housing list, but it’s long. The woman nods, and you can see the moment she stops believing. That moment is the pipeline breaking.
The system often fails not because nobody cares, but because capacity is short and the pathway is brittle. If there aren’t enough beds, enough stabilization slots, enough detox and treatment capacity, enough supportive housing units, the system becomes triage.
Triage isn’t a pathway. Triage is a holding pattern.
Then there’s the assumption problem. Many help systems assume a person can behave like a housed person. They assume you have a phone, an ID, a place to store documents, transportation to appointments, the ability to keep track of dates, and the mental stability to tolerate waiting and setbacks. Those assumptions collapse quickly when someone is living outside.
This is why people fall through gaps even when “services exist.” Shelters can also be mismatched to reality. Some are crowded and stressful. Some feel unsafe. Some have strict schedules that make employment harder. Some separate couples. Some exclude pets. Some exclude active substance use, which means the people at highest risk of overdose are often the people least able to access shelter. If the “help” feels worse than the street, people avoid it, and the public calls that refusal “choice.”
Sometimes it is choice. Sometimes it’s risk management.
Another delivery failure is coordination. A person can be eligible for housing but not connected to treatment. They can be connected to treatment but discharged into homelessness. They can be in shelter but lose the bed if they miss a meeting. They can be arrested for a minor offense, lose everything, and restart the whole process from zero. When systems don’t share responsibility, the person becomes the only one expected to coordinate the maze while also surviving.
Then we hit burnout. Frontline workers are asked to hold impossible ratios and impossible expectations. They burn out. They leave. Programs churn staff. Relationships reset. Trust resets. The pipeline gets weaker, not because the workers are weak, but because the workload is constant crisis. This is also where the “we spend so much and nothing changes” frustration takes root. A large share of homelessness spending happens in the most expensive part of the system: crisis response. Ambulances. ER care. Hospital boarding. Policing. Jail. Sanitation. Court time.
It’s not that money isn’t being spent. It’s being spent on churn because stable capacity isn’t there.
So what does a serious delivery fix look like?
It starts with capacity, but not vague capacity. The right capacity in the right order. You need low-barrier stabilization so a person can get safe quickly. You need mental health crisis options that exist in reality, not only in theory. You need detox and treatment slots that are accessible. You need supportive housing for those who can’t maintain stability without ongoing support. You need prevention tools for those who are still housed but one step away from collapse.
Then you need workflows that match street reality. Simplified intake. Fewer documentation barriers. Better data sharing and coordination. Case management that isn’t spread so thin it becomes a referral machine. Transportation support. Safe storage options. Anything that reduces the friction between a person and the next step. Finally, you need accountability measured by throughput. Not how many people were “engaged.” Not how many flyers were handed out. How many people exited to stable housing. How many stayed housed. How many stopped cycling through ER and jail. How many blocks stopped functioning as open-air waiting rooms.
Part 6 isn’t glamorous, but it’s where success actually lives. The pipeline is the difference between a city that keeps people moving toward stability and a city that keeps people marinating in crisis.
Part 7 is where it gets hardest, because even if the pipeline improves, a society still has to decide what it will enforce in public space, and how to do it without losing legitimacy.